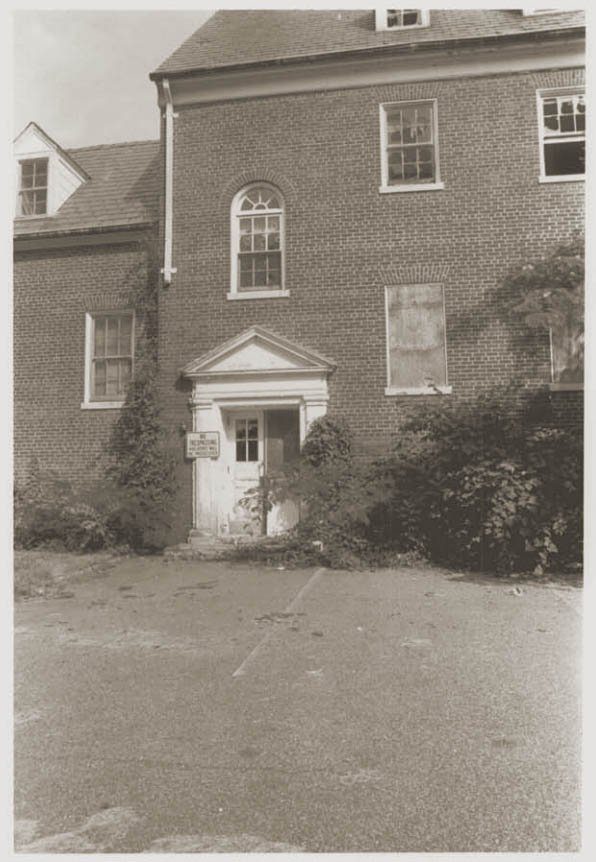
Thirty minutes east of Washington D.C., a collection of brick buildings are deteriorating on a sixty-acre campus buried in a residential pocket of Glenn Dale, Maryland. A foreboding appearance supports local lore of ghosts haunting a former insane asylum, although the truth is more benign. The Glenn Dale Sanatorium was the government’s post-Depression answer to fighting tuberculosis among the working class in the nation’s capital. The hospital’s service life was cut short by advancements in medicine, which eventually forced the facility to close its doors before its fiftieth birthday.
Multiple attempts to sell the remaining tract to a developer have been thwarted by a well-meaning law designed to protect the buildings and preserve Glenn Dale’s quiet, pastoral landscape. Some of the structures are still salvageable, but asbestos abatement alone could approach $5 million dollars.
If the former hospital is to be saved, its rescuer must have deep pockets, and certification to operate a continuing care retirement community.
Tuberculosis (TB) is an infectious disease that attacks the lungs; if left untreated it can cause death. The disease is spread through the air, and symptoms include a chronic cough with blood, fever, night sweats, and weight loss.
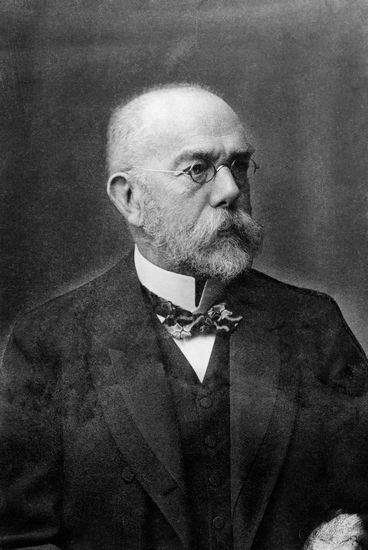
The disease wasn’t officially discovered until 1882 by German Dr. Robert Koch, with recent evidence suggesting the disease has plagued humankind as far back as 4,000 BC. Spinal infections found in Egyptian mummies reveals tuberculosis may have been widespread in ancient Egyptian society. Ancient Greek physician Hippocrates noted the infection, then referred to as “consumption,” was the most widespread and fatal disease of his time.
Mycobacterium tuberculosis also became widespread throughout Europe during the Industrial Revolution. During the 17th and 18th centuries it is estimated one quarter of all adult deaths were related to TB. Over time disease has claimed the lives of many well-known figures in history: Frederic Chopin, Franz Kafka, Henry David Thoreau, King Tut, John Keats, Edgar Allen Poe, George Orwell, Doc Holliday, and Eleanor Roosevelt, among many others.
At the dawn of the twentieth century in the United States, tuberculosis infection was at risk of becoming an epidemic. At the time there was no cure, only a generally-subscribed regimen of fresh air, sun, and a bucolic isolation from society. For decades, municipalities around the country scrambled to erect aesthetic hospitals with verandas in pastoral locations to treat those suffering from the disease.
By 1930 tuberculosis was the most deadly contagious disease in the United States, with a mortality rate of 71 per 100,000 people.
*
TB Hospital for DC
Children’s tuberculosis poster, circa 1930. (source)
Washington D.C. had the fourth-highest rate of tuberculosis deaths at the dawn of the twentieth century. The district’s first sanatorium was built in 1907, and by the 1920s it was overcrowded. The District did not have separate facilities for children, who were physically weaker hosts of the bacteria and faced a greater threat. In 1924 the Tuberculosis Association of D.C. filed a report with the commissioner outlining the need for a children’s tuberculosis sanatorium. Three years later the Monday Evening Club filed a similar document with the Bureau of Efficiency.
The wheels started rolling in 1929, on the cusp of the Great Depression. Bills were introduced in both the House and Senate authorizing $500,000 for the construction of a children’s tuberculosis sanatorium to serve the D.C. metro area. President Calvin Coolidge passed the bills three days before leaving office, on March 1st, 1929. Later a feasibility study was performed, after which the appropriation amount was increased to $625,000. Authorization for this increase was given by President Herbert Hoover on April 8th, 1930.
Once funding was arranged officials searched for a place to build the new children’s hospital. As many as 122 sites in D.C., Maryland, and Virginia were considered. In August and September of 1930, District commissioners purchased 156 acres from Margaret R. Sherman for $52,650 (parcel 153, 359/16) and 60 acres from Daniel B. and Anna Belle Lloyd (parcel 124, 359/18) for $15,250.
Glenn Dale’s Children’s Hospital building, eighty years later. (courtesy Mike Perry)
There was little development, a 1914 topographical map shows just four homes were on the primarily forest-covered lands. The combined 216-acre parcel in Prince George’s County was just fifteen miles northeast of the District of Columbia. It was comparatively remote, but reachable – both the defense highway (Annapolis Road) and the railway provided access.
Tasked with designing the new campus was D.C.’s Office of the Municipal Architect, at the time led by Albert L. Harris. He was advised by hospital design specialists such as NYC’s Thomas B. Kidner and Detroit’s Dr. Henry D. Chadwick, who suggested the hospital be located outside of city limits – partially for the quiet pastoral setting, but also to reduce the children’s pain from family separation.
Seven generations of plans were reviewed before a winner was chosen in July of 1931. By October of that year plans for a Colonial Revival/Georgian style were approved by the hospital committee. Lawrence Johnston, also of the D.C. Municipal Architect’s Office, was credited with the design of the children’s hospital and nurse’s building.
Construction of the children’s hospital was completed in 1933, however the first patients were not admitted until the hospital officially opened on September 15th, 1934. When it opened, Glenn Dale included the children’s hospital building, the nurse’s dormitory, a power plant, and an old residence that belonged to a former property owner. Known as the Randall House (and formerly the Duvall-Meriken residence), it was located northeast of the children’s hospital building and served as the superintendent’s house until a new superintendent’s residence was built in 1935.
The original design of the children’s hospital called for 150 beds. In the spring of 1933 this was increased with a $400,000 appropriation from Congress to enlarge the building. Attached to the bill was another appropriation of $100,000 toward the planning and design of a 400-bed adult sanatorium.
A Public Works Administration (PWA) grant of $1,500,000 was approved to fund construction of the adult sanatorium and its associated buildings (doctor’s quarters, nurse’s dormitories, garage, laundry, power plant, etc.)
The $400,000 children’s hospital expansion was completed by 1936. The addition of the wings increased capacity to 300 beds and gave the formerly rectangular building a new “U” shape.
Between 1936 and 1937 two Work Projects Administration (WPA) murals were added to the children’s hospital. The first, painted by Bernice Cross, depicted Old King Cole and other Mother Goose characters; it was on the left side of the lobby and was missing during a 1987 survey. It is believed to have been painted over or removed.
Another mural was added by artist Allan Page Flavelle in 1937, painted on the ceiling of the heliotherapy room of the second floor of the children’s hospital. Flavelle’s mural depicted the history of electricity, however it was painted over before it was finished because hospital administration felt it was “incomprehensible” and taking too long to complete.
After three years of planning and construction, the adult hospital at Glenn Dale Sanatorium opened on September 15th, 1937 with beds for 400 patients. It also contained classrooms, a dentist’s office, a medical library, operating rooms, an x-ray laboratory, and a heliotherapy room. Along with its new facilities, the hospital boasted expansive rolling lawns. Glenn Dale Hospital’s lush, manicured landscape earned it the nickname “Glenn Dale Golf Club.”
Surgeon General Thomas Parran Jr. called Glenn Dale Hospital “the most up-to-date and complete institution of its kind in the country.” On the roof of both hospital buildings were sun decks for heliotherapy. On cloudy days patients would get their vitamin D while parked underneath ultraviolet lamps. Was it safe? Period literature attempts to assuage concerned parents. One pamphlet read:
“Children will glow and tingle with the soothing substitute for Mr. Sun.”
Glenn Dale’s first superintendent was Dr. Daniel Leo Finucane (b.1903, d.1984), who served in such capacity from 1934 until he was appointed Director of Public Health for the District of Columbia in 1957. The hospital thrived under Dr. Finucane for the twenty-three years he was in charge. He received accolades for his whitepapers, including his 1941 release of “Pulmonary Actinomycosis Complicated by Pneumothorax Treatment.” (1.5 MB pdf)
There were also unfortunate incidents at Glenn Dale that made the news. In the 1940’s a series of Congressional hearings over the quality of care at Glenn Dale uncovered patients reported finding fingernails in their food. In 1948 a Glenn Dale TB patient had the wrong lung collapsed during a thoracoplasty due to a clerical error. A thoracoplasty involves surgeons removing one or more ribs to allow a diseased lung to collapse and rest (pictured).
In the case of the Glenn Dale patient, she was suffering a “very serious tubercular condition” in her left lung. Glenn Dale surgeons were mistakenly directed to remove her right ribs, partially collapsing her healthy right lung. Dr. Finucane told reporters the patient’s condition was serious, but emphasized that it was “not attributable to the error.”
Finucane stepped down from his position at Glenn Dale Hospital in 1957 to accept the position as Director of Public Health of the District of Columbia. By this time Glenn Dale Hospital had grown to its current size. Topography maps from this era show the hospital’s campus appears similar to how it exists today, the only notable omission being the missing incinerator building, which was added later in 1960.
1977 aerial map of Glenn Dale Hospital (courtesy Mike Perry)
In honor of the long-serving superintendent, the U-shaped employee dormitory building adjacent to the Adult Hospital was re-named Finucane Hall (pictured below).
Eastern elevation of Finucane Hall, circa 2012.
By the late 1950s, advances in medicine had allowed tuberculosis patients to receive treatment in their homes. There was no longer a need for large institutions on 100-acre campuses, removed from the city. This fueled suggestions in 1957 to sell the Glenn Dale facility in order to fund a larger expansion of D.C.’s General Hospital complex. However discussion never got off the ground and Glenn Dale remained open.
[ At its peak Glenn Dale Hospital was home to more than600 patientsand employed nearly 500 workers from many fields, from physicians and nurses to cooks and maintenance workers. ]
The advancements in treating tuberculosis forced Glenn Dale to shift its operational focus, and in January of 1960 the hospital opened to persons with any chronic or long-term illnesses. By 1965 about one third of the patient population was being treated for non-TB ailments, including cardiovascular, musculoskeletal, respiratory, and digestive disorders.
*
“New Experiences for Tuberculosis Patients in Occupational Therapy” booklet, published by the District of Columbia Tuberculosis Association, circa 1964 (source)
The luster of Glenn Dale’s “state of the art” moniker had worn off by the 1950s; by the middle of the decade the hospital appeared “dingy and bleak.”
Glenn Dale did offer activities for its patients, including bingo, card games, weekly movies, and even typing classes. Those who were able, were offered part-time jobs in the hospital canteen. Patients could have visitors, but they were not allowed to hug or kiss loved ones. And while the landscaping and roaming paths of Glenn Dale were beautiful, patients were not allowed on the grounds.
The patient handbook offered additional advice: “Stay indoors on damp, rainy days. Discard your used tissues in a paper bag to be burned. Do not kiss anyone.Stay away from children.”
[ Did You Know? In 1939 Glenn Dale’s Bessie Crocker became thefirst African-American nurseto work at a D.C. municipal hospital. ]
Effective medicinal treatment did not come until 1943, when researchers at Rutgers University discovered the antimycobacterial drug streptomycin. The following year a Swedish chemist developed para-aminosalicylic acid (PAS), which in 1948 was determined to be a more effective treatment. A third treatment, isoniazid, was released to the market in 1952.
Glenn Dale began using PAS treatments in 1948; each morning patients were given a small cupful of the brackish concoction. While the drug effectively reduced TB deaths, its regimen required patients to increase their stay by up to two years. By 1954 the average stay at Glenn Dale Hospital lasted 482 days; this increased the size of Glenn Dale’s waiting list, which that year had reached 245 names. Hospital wards were originally segregated by race and sex, however by the 1950s available beds were issued to the next patient on the waiting list regardless of race or gender.
In 1958 the hospital added a locked detention ward for runaways and uncooperative patients. The following year a Glenn Dale patient was fined $500 and given a one-year jail sentence for running a lottery.
[ In 2006 author Leah Y. Latimer’s “Quarantined”described the tribulations of her mother during a stay at Glenn Dale Hospital. Latimer’s acclaimed story gives an inside look to how suspected TB patients were treated at Glenn Dale in the mid-twentieth century. ]
Glenn Dale’s grounds are still beautiful, even in decay. (courtesy Mike Perry)
*
Glenn Dale Discoveries, Luminaries, and Pioneers
In its later years Glenn Dale fostered ideas and creative solutions to various maladies. In 1965 Glenn Dale’s Dr. James W. Barnes Jr. made national news when he reported a successful way of treating skin ulcers at the third annual Scientific Assembly of the Medical Society of D.C. His treatment was a surprisingly simple redux of the old method of applying ordinary table sugar directly to the ulcer cavity, then firmly covering the wound with an airtight dressing.
“The way sugar works is toform a counter-irritation, so the original wound is changed. It appears to initiate wound repair by causing ‘local injury’ and be a stimulus for granulation tissue formation.”
– Dr. James W. Barnes Jr., Glenn Dale Hospital
Across the previous twelve years Dr. Barnes claims this method cured 41 of 49 patients suffering ulcers at Glenn Dale. Barnes, who was a treatment physician and not one who plied his trade in research, acknowledged additional studies should be conducted. “I am sure that enzymes are involved, butI have never had time to do the research.” Dr. Barnes would eventually find acknowledgement for his discovery in a 1966 issue of Popular Mechanics and from the American Medical Association in 1973.
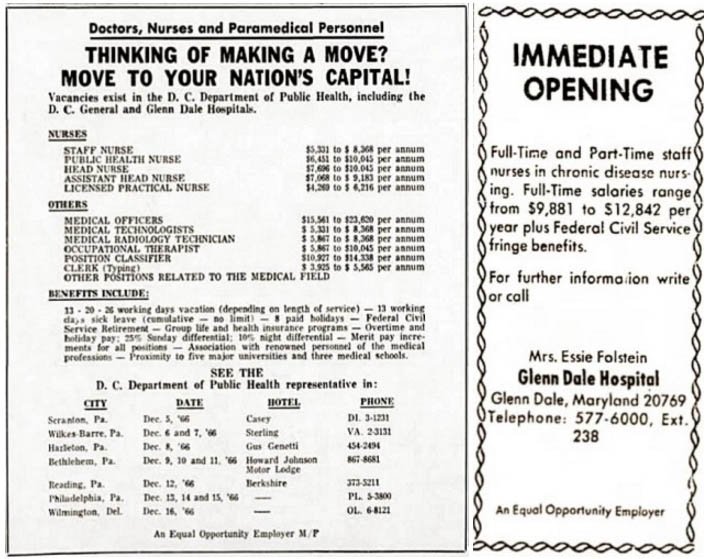
Glenn Dale Hospital “Help Wanted” ads from 1966 & 1970
In 1969 Dr. Tunkur Madhu, chief of physical medicine and rehabilitation at Glenn Dale Hospital, was sharing his technique of injecting boiling water around the spinal cord to bring paraplegics relief from spasticity of the legs. Dr. Madhu’s procedure had been successful for twelve patients as was described in the Journal of theAmerican Medical Association.
And there is the story of Bertha Smith, a blind teacher at Glenn Dale Hospital who invented a new reading system for the blind in 1971. She developed the system to help the elderly blind and those with missing extremities or sensitivity issues. Smith’s system uses Braille characters 2.5 times larger than the original Braille system, which dates to 1824. Bertha’s project was subsidized by the Veterans Administration, who adopted her “Jumbo Braille” system in 1971 at the request of disabled Vietnam veterans. While Jumbo Braille is not still widely used today, it does find use as a fingertip sensitivity learning tool for the recently blind.
Glenn Dale Adult Hospital Building in 2016 (courtesy Mike Perry)
*
End of the Road for Glenn Dale
In the early 1970s the original structures at Glenn Dale Hospital were beginning to show their age. Renovation costs were estimated to be $15 million, about twice the cost of new construction. By 1973 the District considered closing the hospital and moving to a less expensive facility in the city. In the forty years since Glenn Dale had been constructed there were numerous advancements in building safety and changes to the fire code. This was exposed in 1976 when Glenn Dale Hospital failed an inspection and received multiple fire and safety code violations. Among the issues cited were a lack of approved fire exits per floor, no smoke doors, and perhaps most critical, the lack of a sprinkler system.
(courtesy Mike Perry)
By 1978 the hospital was precariously grappling with solvency. Gone were the children, tuberculosis patients, and UV lamps. In their place were 350 Medicaid patients unable to care for themselves. The estimated renovation bill – now with fire and safety upgrades – had ballooned to $20 million. Each time the estimate grew, a Glenn Dale renovation appeared less likely to happen.
Glenn Dale Hospital was officially closed in January of 1982 by D.C. mayor Marion Barry. The hospital’s final Chief Medical Superintendent was Dr. James Wills, who had been with the organization since he was a staff physician in 1965. As to the hospital’s original mission, Dr. Wills revealed that between 1965 and 1980, no child in the facility died as a result of tuberculosis.
A battle over control over the site ensued between the District and the United States General Services Administration (GSA). The former wanted to sell to a developer while the latter claimed the former hospital was Federal property, and had only been leased to the District. A review of deed information showed the United States of America had acquired the two parcels to form Glenn Dale in 1930.
In October of 1984 a U.S. District Court ruled in favor of the District, however the District did not receive full control until Representative Steny H. Hoyer (D-Md.) enacted legislation in October of 1988. Still, the District did not officially acquire the property until 1989. Initially, the District was asking “no less than” $10 million for the 209-acre parcel.
Glenn Dale’s Adult Hospital, 2016 (courtesy Mike Perry)
In the six years since Glenn Dale had closed there were several proposals for re-use, including a District jail, drug treatment facility, and landfill. None of these options sat well with the surrounding communities, which combined with a murky ownership situation, prevented any proposal from getting past the drawing board.
Seven years after the hospital closed, the first strong proposal came into focus. In the spring of 1989 it called for a 10-acre health spa and retreat for city employees. It would cost $19.2 million to build and was partially-funded through a proposed tax increase. Concerned about the city’s deficit and funding gaps, the D.C. Council quashed the plans. Another proposal which featured homes and limited commercial development was also rejected due to cost and density.
Glenn Dale Children’s Hospital (courtesy Mike Perry)
Prince George’s County officials began showing interest, and by September of 1990 a deal was announced: The County would pay $3.95 million for the 209-acre site, funded via the County’s property tax revenue.
The land would remain undeveloped, according to Prince George’s officials, due to the wishes of neighbors to keep the land as open space. Not accounted for in the sale price were the estimated $2.3-$4 million in asbestos removal costs.
In late 1993 the District of Columbia hired PMT & Associates to conduct an environmental assessment of Glenn Dale Hospital. In their January 1994 Phase I Environmental Assessment (15 MB pdf), PMT observed that “elevated levels ofradon” had been reported in the area and that the hospital buildings “generated special medical wastes, used radiation (X-ray) equipment, and maintained a paint shop on site.”
[ Radon is a radioactive gas which occurs naturally during the breakdown of uranium. It is heavier than air and will usually settle at lower levels. Radon often enters old structures with other soil gases through cracks in the slab and foundation floors, cinder walls, slab joints, floor drains, and sump pumps. Similar to the effect of opening the flue to a fireplace, a pressure differential called thestack effectdraws gases into the buildings from the ground. ]
Due to the paint shop, the PMT communique suggested a lead paint survey be conducted to evaluate what lead abatement measures might be necessary. The report also broke down Glenn Dale Hospital’s Asbestos Containing Material (ACM) into three forms:
Friable ACM:Can be crumbled, pulverized, or reduced to powder by hand pressure. (Found in joint compound, wall board, ceiling tiles, pipe insulation material, tank insulation.)
Category I Non-Friable ACM:Still in solid form. Resilient floor coverings (like vinyl tile), asphalt roofing products, packings, and gaskets. Also found in gasket and roofing materials.
Category II Non-Friable ACM:Not as resistant to crushing or pulverizing as Category I; more likely to become friable.(Such as cement board, cloth connections, cement-board siding, and corrugated roofing and siding).
Because it is brittle and easily crushed, friable ACM is considered the most immediate threat. The report recommended that friable ACM be removed prior to any renovation, and suggested the cost for such an operation could approach $2.4 million. In the steam tunnels ACM was so pervasive removal was not practical; it was suggested the tunnels be sealed off instead.
This floor tile is an example of friable ACM. (source)
*
Glenn Dale under M-NCPPC
1995 Deed for Glenn Dale Hospital
In 1994 Maryland House Bill 113 [ch. 361, § 1] authorized a transfer of Glenn Dale ownership to the Maryland-National Capital Park and Planning Commission (M-NCPPC) for an as-yet undetermined fee. The M-NCPPC is a state agency, created in 1927 to handle the jurisdiction of parks and planning in both Montgomery and Prince George’s counties.
The House bill required the M-NCPPC to maintain 150 acres as an open park while 60 acres could be sold, rehabilitated, and developed – but only into a Continuing Care Retirement Community (CCRC). In the bill only four Glenn Dale buildings (children’s hospital building, adult hospital building, Capper Hall, McCarran Hall) were required to be rehabilitated for reuse; the remainder would be slated for demolition.
The bill was passed in 1994, however the deed wasn’t signed by Mayor Marion Barry until March 31st, 1995. The deed filing (201 Kb pdf) stated the M-NCPPC paid $4,105,664 for the property, and included an interesting twenty-year “excess profit” covenant which recently sunsetted in 2015.
Eastern elevation of Peabody Hall and wing of Children’s Hospital, 2016. (courtesy Mike Perry)
District officials were expecting the transfer of Glenn Dale would spur action, however the House bill’s clause requiring a Continuing Care Retirement Community ultimately encumbered development. Most developers were not specifically qualified to operate a CCRC; those that were qualified to operate a CCRC lacked the necessary financial backing.
[ In November of 1997 Glenn Dale Hospital was added to Maryland’s Inventory of Historic Properties (P.G. #70-50) ]
In January 2004 the M-NCPPC commissioned a property survey and map of the property. The following month the Maryland General Assembly discussed proposed House Bill 841, which proposed to relax the 1994 laws on the Glenn Dale property. The bill would have allowed the M-NCPPC to develop single-family housing, or a combination of a CCRC and single-family housing:
“The Commission may sell, lease, or otherwise transferthe approximately [60] 105 acres to a person who will use the property as a continuing care retirement community in accordance with Article 70B, §§ through 23 of the Code OR FOR SINGLE-FAMILY HOMES OR A COMBINATION OF A CONTINUING CARE RETIREMENT COMMUNITY AND SINGLE-FAMILY HOMES.”
(courtesy Mike Perry)
This less-restrictive bill allowed the M-NCPPC to sell the outside reaches of Glenn Dale’s acreage to single-family home developers, which they did, leaving the 60-acre parcel that exists today.
In 2005 the M-NCPPC sought and received four bids to redevelop the remaining property, however nothing materialized. Two years later the director of Prince George’s County parks and recreation said the County had not set aside money to establish the park at Glenn Dale, nor did they have a timetable for developing the retirement center. The General Counsel for the M-NCPPC sent a letter to the D.C. Attorney General asking to be released from the twenty-year “excess profit” covenant that was attached in 1995.
“The commission has NO INTEREST OR DESIRE to change the law as it relates to the property… If we can’t reach an understanding with the District, we’ll have to wait till time runs out on the covenant.”
– Adrian Gardner, General Counsel M-NCPPC
The excess-profit covenant expired in 2015.
Children’s Hospital building, Glenn Dale Sanatorium. (courtesy Mike Perry)
In October of 2008 a Community Advisor Group meeting was held to obtain the pulse of Glenn Dale’s neighbors. Group members were not amenable to the single-family homes development and instead favored restoring the buildings and using the property for a CCRC as mandated in 1994’s House Bill 113. According to M-NCPPC senior planner Carol Binns, since the commission acquired the property in 1995, no one had come forward to present a plan to build a CCRC facility. In February of 2010, Binns divulged that the roofs of the main buildings had been compromised, and that the roof of the nurse’s dormitory had completely collapsed during the winter snow storms of 2010.
The M-NCPPC attempted another sale in June of 2010, again asking developers for proposals for the 60-acre parcel. With six bidders in the mix the deadline was extended to October. The excess-profit covenant was undefeatable for most, leaving the commission with two bids by the deadline. Both were rejected because neither bidder was licensed to operate a CCRC.
Preservationists put another foot forward in September of 2010, when the Glenn Dale community and Citizens Association asked the county’s Historic Preservation Commission that Glenn Dale Hospital be listed on the National Register of Historic Places. The nomination was the culmination of a two-year process, and when awarded, would offer potential Federal and State subsidies and rehabilitation tax credits to any perspective purchaser.
(courtesy Mike Perry)
In December of 2010 County Executive Jack B. Johnson offered his approval to the recommendation. Glenn Dale Hospital was officially listed on the National Register of Historic Places on November 18th, 2011(#11000822). Preservation Maryland placed Glenn Dale on its list of threatened historic properties in 2014.
– Henry Wixon, president of Glenn Dale Citizens Association
*
Site Assessment, Survey, & Market Study
KCI Technologies produced a Glenn Dale Hospital Asbestos-Containing Materials Report (15 MB pdf) for the M-NCPPC in April of 2013. The Phase II Environmental Site Assessment (ESA) exposed a laundry list of concerns that eclipsed the warnings of the 1994 Phase I assessment. Notable in the report:
There are four above-ground storage tanks, at least eight underground storage tanks, and another eighteen storage tanks associated with the site’s steam heating system.
Two above-ground diesel storage tanks on site should be immediately pumped. Both are reservoirs for the emergency generators in the children and adult hospitals. Another above-ground tank is next to the incinerator and held its fuel. The fourth was located next to the paint shop and used for storing used paint and chemicals.
There are undocumented underground storage tanks (USTs) on site.
There is approximately 1,160 gallons in three of the USTs that needs to be removed, however the three largest USTs could not be accessed or evaluated.
In total, an estimated 10,000 gallons of liquid will need to be removed.
Tank 1 can be sealed in place, however complete excavation and removal of tanks 2-6 was estimated to cost between $50,000 and $80,000.
USTs 5 & 6 sit at the foot of the smokestack of the heating and power plant; excavation and removal would threaten the building and smokestack integrity.
Three wells are located at Glenn Dale. One is southwest of Finucane Hall, drilled to a depth of 798 feet. Another was drilled to 316 feet, near the sewage treatment building. The deepest is 946 feet, next to the water tower. The wells tap into the Patapsco aquifer and if they haven’t already, are at risk for future groundwater contamination.
Map of Glenn Dale’s steam tunnels
The eighteen tanks of the steam system don’t pose an immediate environmental threat, but the insulation around the tanks’ piping is asbestos containing material.
KCI also identified asbestos-containing pipe insulation in the steam tunnels under Glenn Dale that connect most of the buildings to the central heating plant.
Asbestos abatement for all buildings on site could cost between $4.4 million and $5.4 million dollars. Further building deterioration over time will increase these costs. (jump to individual building assessment section)
Summary of Glenn Dale Asbestos Cleanup Estimates
[ What’s the deal with asbestos? It’s a set of six naturally-occurring silicate minerals. Because asbestos is corrosion-resistant, incombustible, and strong, it was popular in many commercial building products for nearly 100 years. In the 1930’s it was still an accepted material as its dangers were not yet understood. It is commonly found in ceilings, floors, walls, and plumbing, and was most often used as an insulator or to strengthen cement and bonding agents. Over time exposed Asbestos fibers can become brittle and when airborne, are inhaled into the lungs. Prolonged exposure can cause severe ailments including chronic lung disease, lung cancer, and Mesothelioma. The U.S. Consumer Product Safety Commission banned the use of asbestosin the late 1970’s; the Environmental Protection Agency followed suit in 1989. ]
Glenn Dale now has security cameras.
In August of 2014 citizens asked for better security and stronger cleanup efforts at the Glenn Dale Hospital campus. Representative James W. Hubbard revealed that no one has been able to raise the $7 million necessary to clean up the site: “It’s an expense that haschased interested parties away.”
Regardless, site cleanup and security has begun in earnest. In 2015 some of the land was cleared of debris and grass cut back, and there was also a mention of cameras being installed on the property.
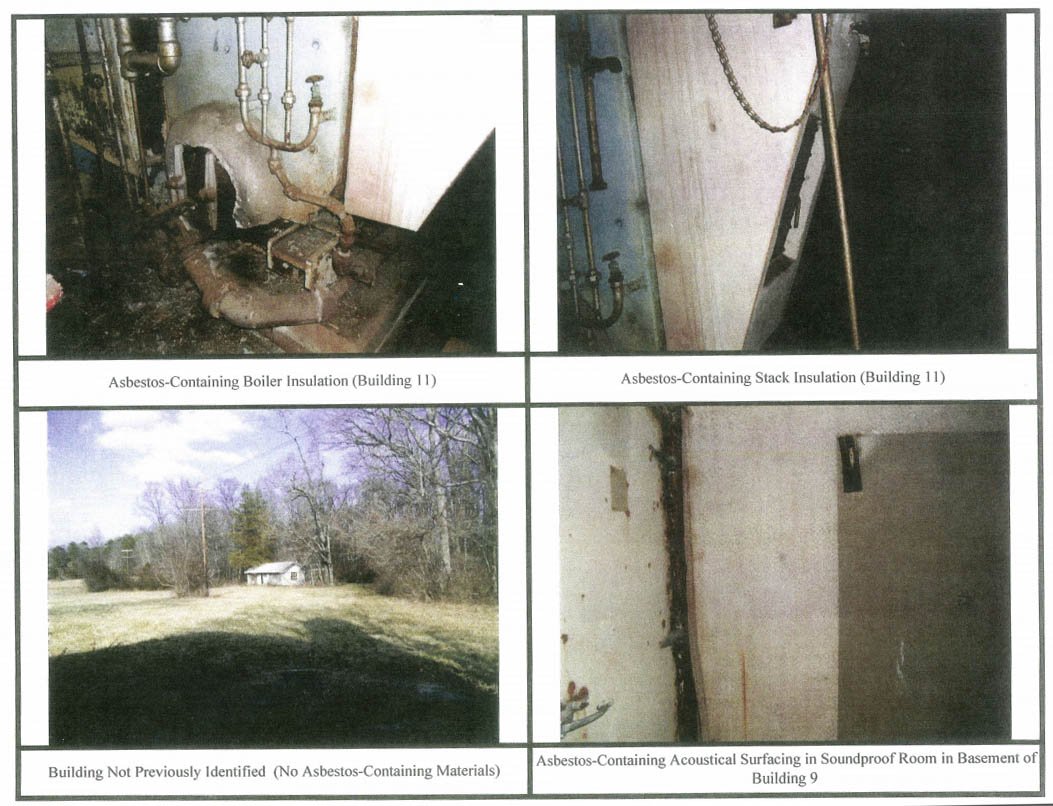
Photographs of Glenn Dale’s asbestos contamination
(courtesy KCI Technologies & Prince George’s County)
*
A Field Observations Report (22 MB pdf) was performed on April 16th, 2015 to determine the feasibility of mothballing the structures. Mothballing is a process that involves temporarily sealing a building to protect it from weather and vandalism while it awaits reuse. It is not inexpensive and can call for major repairs costing upwards of 10% of an overall renovation budget.
Before a building can be mothballed it must be evaluated and stabilized. First and foremost, foundation and roof repairs must be made; if they cannot be repaired the building will not benefit from mothballing. Next all entrances and windows should be sealed to keep moisture and pests outside. Once a structure is stabilized it can be properly mothballed. The steps in this process are securing the buildings, providing adequate ventilation, and establishing an on-going maintenance and monitoring program.
Stage in the Adult Hospital’s auditorium: 1989 (top) & 2016 (bottom)
(courtesy Mike Perry)
The Glenn Dale Hospital mothballing feasibility report was released on June 8th, 2015, with the following notable observations:
Most of the window glass has been broken.
The brick parapets on the Children’s Hospital haveGlenn Dale Hospital roof damage.
been removed by scavengers to steal the metal flashing. Thieves have also removed rain gutters and leaders.
A significant amount of brickwork and roof repair would need attention before mothballing.
The remaining wooden structures and porches are in poor condition and may need to be disassembled to ensure survival.
Invasive vegetation covers many of the buildings.
The porch on the rear of McCarren Hall has completely collapsed and damaged the surrounding building fabric. A large opening was created when the porch pulled away from the roof, allowing water to infiltrate the building.
The porches on the polygonal additions of the Adult Hospital wing are severely deteriorated and may be beyond repair.
The porches on Capper hall have severe roof damage allowing water infiltration.
Wooden pergolas at Gibson Hall and Peabody Hall are in poor condition and will have to be removed.
The flat roofs of the Apartment Buildings have completely collapsed; survival of these buildings is questionable. The flat roof of the arcade has also begun to collapse. (jump to mothballing evaluation building-by-building)
The roof of the Adult Hospital at Glenn Dale Hospital.
*
In August of 2015 a market study was conducted to evaluate the former Glenn Dale Hospital site as a CCRC (original pdflink now dead, 19 KB document transcription here). Specifically, the study sought to “evaluate if market depth and community receptivity are favorable for the reuse of the Glenn Dale Hospital campus as a Continuing Care Retirement Community (CCRC).”
The market study’s observations:
There is market demand for a CCRC at the Glenn Dale Hospital site.
Exceptional growth was projected in affluent seniors.
There is a lack of contemporary retirement offerings within or proximate to the MA.
However it is recommended to have an architectural and engineering adaptive reuse assessment, as well as a financial feasibility analysis.
Citing the lack of the two aforementioned assessments, the report was ultimately ineffectual: “It is not possible to make a specific conclusion that a CCRC could be successfully redeveloped and operated at this site.”
*
Glenn Dale Hospital Today
Open-air hallway in the Adult Hospital building. (courtesy Mike Perry)
In March of 2016 the County Redevelopment Authority (RA) issued another solicitation seeking developers to take on the former Glenn Dale Hospital, vacant for the last 34 years. The RA hopes to have a development agreement in place by August of 2017. Latest estimates had redevelopment costs approaching $200 million.
Former student Caitlin Chamberlain featured Glenn Dale Hospital in her 94-page master’s thesis. She notes the hospital’s worst enemy is nature, which is causing the buildings to decay at an alarming rate.
Chamberlain argues the law requiring a CCRC is actually preventing development. “To have that just one specific use is so limiting. Nobody benefits from a law that is too restrictive.”
Capper Hall circa 2016 (courtesy Mike Perry)
Also working against Glenn Dale are rehabilitation costs, specifically labor. Chamberlain cites a comment from the developer of Avalon Danvers, who estimated the rehabilitation cost at Danvers State Hospital was “two and a half times as expensive as new construction.” This rhymes with comments by Massachusetts Associate Planner Gene Bunnell in Built to Last: A Handbook on Recycling Old Buildings. In his book Bunnell estimates the process of renovating old buildings is five times more labor intensive than new construction.
There are other thorns with which to contend. Because Glenn Dale sits on an approved Historic Site, developers would need an approved Historic Area Work Permit (HAWP). This permitting process allows the Historic Preservation Commission to ensure any proposed construction aligns with the historic integrity of the property.
Finally there are the issues of parking and traffic. The property sits in an upscale residential area with a bucolic backdrop along a quiet, two-lane Glenn Dale Road. Local streets offer no parking and would not support a commercial thoroughfare. Construction of a large parking lot and widening of the roads would be incongruous with neighbors’ requests the site maintain its residential landscape and forested backdrop.
Western elevation (rear) of Adult Hospital Building, 2016. (courtesy Mike Perry)
*
Virtual Tour
Glenn Dale Hospital is about 30 minutes east of the District of Columbia via US-50. For the road less traveled, the smaller 704 to the east (Martin Luther King Jr. Highway) will turn into Annapolis Road before dropping you at Glenn Dale’s doorstep. Turn left onto Glenn Dale Road when you see the old white water tower and on your left you’ll pass neighborhoods with upscale, $500,000 homes.
After about one thousand feet the windowless red brick wall of a large empty building peeks above the crest of a hill on the right (Google Streetview). This is the west wall of the Children’s Hospital Building, one of the largest and oldest buildings on site. Keep driving and you realize Glenn Dale Road bisects the campus; on the left in the distance you see the outline of the Adult Hospital Building and to its left Finucane Hall, a former employee dormitory named for the hospital’s first superintendent.
Just to the right of Glenn Dale Road and directly between the two large hospitals sit a pair of smaller buildings connected by a brick arcade. Capper Hall (former children’s nurse dormitory) abuts the road and is connected by a walkway (pictured below) to the perpendicular McCarran Hall (former adult’s nurse dormitory), which is partially hidden from the road behind trees.
Glenn Dale Hospital arcade in 2016 (courtesy Mike Perry)
Because of its location, Capper Hall has easy, obvious access points. However a County law enforcement officer who lives in the trailer directly across the road will not hesitate to issue criminal citations to those caught trespassing.
Despite the extra security, in recent years one of the entrances to Glenn Dale’s grounds has been used as a household refuse and tire dump.
Metal scavengers have combed through the buildings and removed everything from the copper metal flashing to downspouts and plumbing. The resulting exposed friable ACM sits in smashed sections of wall board and torn insulation. Unauthorized activity is evidenced by the presence of broken beer bottles and empty packs of Newports. The usual hallmarks of decay are present: Mold, corroded fixtures, peeling paint, and broken glass.
A stroll through Glenn Dale’s buildings today reveals an OSHA nightmare. Ceiling beams sag. Exposed rusty metal rebar grabs the shirt of every careless passerby. Thousands of lead-infused paint chips peel themselves from the walls, and the ripped construction cloth hanging from the ceiling sends asbestos into the air with every flap in a breeze.
(courtesy Mike Perry)
If you were curious, the asbestos threat is greater in the vandalized buildings where scavengers and vandals have torn up the ceiling and walls, exposing friable ACM and leaving large quantities of pipe insulation scattered about the floors. And that’s not to speak of the numerous underground tanks around the property that still potentially contain thousands of gallons of… something.
Vines penetrate the brick and concrete. Ivy has weaved its way inside the buildings through broken windows and missing doors. In the auditorium dozens of ceiling tiles are scattered about the floor. The walls of the laundry house were collateral damage during a paintball battle. Some lower windows have been boarded, but there isn’t a single unbroken pane of glass anywhere on the property.
Rooms still contain rusty chairs and hospital beds, and antediluvian medical equipment is scattered throughout. Taggers have signed Glenn Dale’s walls like it was a guest book, adding grim phrases such as “Go back please” and “Welcome to Hell.”
Peabody Hall, circa 2016. (courtesy Mike Perry)
Previous visitors have also engaged in some staging for effect: The oven found in the morgue of the Children’s Hospital today was actually moved to its present location from the kitchen.
The basements are connected by a set of tunnels that once contained the steam lines which ran to each building. Today they have several feet of standing water and are infested with, among other things, bats, rats, and trash. Over time vandals have removed doors to the refrigeration units in the morgue in the basement of the Adult Hospital.
At one time each of the refrigerated storage units in the Glenn Dale morgue had their doors. Not anymore. (source)
**
EXTRA CONTENT
**
Architects & Landscaping
The campus opened in 1934 and contains 450,000 square feet of building space. Over the next three years it was expanded and renamed Glenn Dale Sanatorium in 1937. Architects: Albert L. Harris, Nathan C. Wyeth, Lawrence Johnston, Merrel C. Coe, Charles B. McGrew, J.L. Cousens, Francis P. Sullivan. Sixteen of the site’s twenty-three buildings were designed by Washington D.C.’s Municipal Architect’s Office and completed between 1932 and 1939. Design was mostly Colonial Revival, popular during the era.
Credit for who designed what at Glenn Dale is a bit murky. The project began under Municipal Architect Albert Harris, who supervised construction of the first two structures until his death in 1933. After Harris’ death Nathan C. Wyeth assumed the post of Municipal Architect until 1946. Wyeth supervised the design of 14 of the 23 buildings at Glenn Dale. Newspapers of the day credit architect apprentice Lawrence P. Johnson with the original design of the Children’s Hospital and Nurse’s dormitory, however the plans themselves (dated 1931 and 1932) listed his supervisor, Chief of the Architectural Division Merrell A. Coe.
Aerial photo of Gibson Hall, circa 2015.
From 1935 until 1937 the Architect-in-Charge was listed as Charles B. McGrew, who worked with the office of the Municipal Architect from 1931 until 1938. After 1938 the Architect-in-Charge was J.L. Cousens. Francis P. Sullivan was a former partner of Wyeth and the only private architect to have worked on Glenn Dale in the 1930s. Sullivan is credited with the four-story addition to the nurse’s dormitory, a 10-family apartment building, and several other smaller structures on site.
Landscaping was also an important part of the Glenn Dale Hospital. In 1937 Joseph C. Gardner prepared a landscaping plan for the nurse’s dormitories, staff residences, and the terraced lawn south of the Children’s Hospital building. The following year these were simplified in a redesign by August H. Hanson of the National Park Service (NPS). Leonard Bartlett Jr, also of the NPS, prepared the landscaping plan for Finucane Hall.
For the purposes of the National Register of Historic Places, the buildings of Glenn Dale were placed into one of two categories: Contributing and Non-Contributing Structures. Contributing Structures were those built between 1933 and 1959 and contribute to the historic and cultural nature of the site. Non-Contributing structures were built after 1959 and do not contribute to Glenn Dale’s historic and cultural nature.
**
Glenn Dale Buildings & Site Map
Below is the information on Glenn Dale buildings culled from this article’s research. Descriptions below were compiled from news stories, environmental evaluations, site surveys, and witness accounts.
Glenn Dale Hospital site map. Blue structures are contributing, yellow non-contributing. (source)
*
Garage interior (courtesy Billy Perry)
1) Warehouse and Garage(1936, 11,500 sq. ft., map). 2016 Status: Still standing. This one-story structure is part of the northeastern block of maintenance buildings at Glenn Dale, accessed from the Cherry Drive loop. It sits directly across from the power plant and smokestack and is in fair condition. Concrete deterioration has exposed reinforcing bars in some areas, which are now corroded. The floors have pockets of standing water.
Mothballing would be comparatively less work than the other buildings, with a restoration of the waterproofing envelope and proper ventilation sufficient. The warehouse and garage are significant harbors of asbestos, which was found in pipe insulation, ceiling tiles, floor tiles and mastic, window glazing, and roofing materials. Asbestos abatement estimate: $28,840 (demolition) – $67,500 (renovation).
Warehouse interior (courtesy Billy Perry)
*
Water tower and power plant with an intact smokestack, circa 2016 (courtesy Mike Perry)
2a) Heating and Power Plant(1936, 6,824 sq. ft., map). 2016 Status: Still standing. This two-story building features a smokestack along its northern elevation. Visual damage is mostly cosmetic. The area below its steel grate floor is flooded. Mothballing is possible with a repair of the building’s waterproofing envelope and draining the standing water. The Phase II ESA found asbestos throughout, in the pipe and tank insulation, the boiler insulation, the stack insulation, ceiling and floor tiles, transite window panels, and roofing materials. Asbestos abatement estimate: $57,025 (demolition) – $101,100 (renovation).
*
Glenn Dale’s Laundry building (courtesy Billy Perry)
2b) Laundry Building(1939, 6,272 sq. ft.,map). 2016 Status: Still standing. The laundry facility is a large, one-story building attached to the taller power plant building. Its condition is fair, with standing water on the floor and heavy corrosion of the structural steel beams, columns, and girders. The roof is in fair condition. Mothballing would be possible with repair to the roof, trimming the vegetation back from its walls, and an evacuation of the standing water inside. Asbestos contamination was discovered it its pipe and pipe fitting insulation, joint compound, and roofing materials. Asbestos abatement estimate: $26,080 (demolition) – $34,380 (renovation).
*
Pump house
3) Pump House(1937, 1,226 sq. ft.,map). 2016 Status: Still standing. This small, one-story building is in poor condition. Mothballing would require extensive roof repair (or complete replacement), as the Phase II ESA found ACM in the roofing materials. Asbestos abatement estimate: $0 (demolition) – $7,500 (renovation).
*
Water softener house
4)Water Softener House(1937, 668 sq. ft.,map). 2016 Status: Still standing. This one-story building is in very poor condition due a partial collapse of the roof. Much of its original equipment remains in place and is poor condition. All metal surfaces exhibit corrosion. Perimeter façade is cracking and at risk of falling. Mothballing would be difficult without extensive building, masonry, and roof repair. Asbestos was found in roofing materials and window glazing. Asbestos abatement estimate: $500 (demolition) – $4,100 (renovation).
Inside Glenn Dale’s water softener house. (courtesy Mike Perry)
*
Glenn Dale’s Apartment Building 1 (courtesy Mike Perry)
5)Apartment Building 1(1949, 5,892 sq. ft.,map). 2016 Status: Collapsing. AKA “Northern apartment building,” this rectangular two-story, four-unit building sits in an overgrown field adjacent to the water softener house, only a stone’s throw from the laundry building. Glenn Dale’s two apartment buildings were added fifteen years after the Sanatorium opened. These industrial style structures were less ornamental than the Colonial-style physicians housing built years earlier. Apartment Building 1 provided housing to the hospital’s maintenance and service staff.
Today the building has all but collapsed; its roof is gone and floors missing, leaving the structure as an empty shell. Mothballing is unlikely and would be prohibitively expensive, requiring construction of a new roof, new floors, and additional bracing. And its debris pile is far from benign, estimated to contain high levels of friable ACM. Renovation not possible. Demolition Asbestos abatement estimate: $170,000.
*
Apartment Building 2 (courtesy Mike Perry)
6) Apartment Building 2(1950, 6,892 sq. ft.,map). 2016 Status: Still standing. Like Apartment Building 1 this structure was designed in a drab industrial style. It was the second of the two apartment buildings and is slightly larger in size, with an extension from its southern elevation comprising the extra square footage. As with the first apartment building, this structure provided housing to the hospital’s maintenance and service staff. Apartment Building 2 has fared only slightly better than Building 1. It is missing all windows and doors, has portions of the floor that have collapsed, and it is overgrown with vegetation. Façade damage is also high, and it is unknown if this building is in fact structurally sound. Both apartment buildings have basements with standing water.
This building could be mothballed with some roof repair and a restoration of the building’s waterproofing envelope. Asbestos was found in pipe and tank insulation, fire door insulation, roofing materials, and the floor tiles and mastic. Asbestos abatement estimate: $42,560 (demolition) – $54,460 (renovation).
Apartment Building 2 (courtesy Mike Perry)
*
(courtesy Bing maps)
7a) Children’s Hospital Building(1933, 125,000 sq. ft.,map). 2016 Status: Still standing. This four-level building (3 floors + basement) was the first structure built and sits on Cherry Drive, the interior loop road of the campus. The Children’s Hospital originally included just the central portion in its original design, and in 1936 the angled wings were added via a $400,000 appropriation by Congress. The center of the building contains a pyramidal slate roofed tower. Two residence dormitories were added years later (Gibson Hall & Peabody Hall), each extending northward from the hospital and encircling the parking lot.
Some of the more obvious non-structural damage to the Children’s Hospital is the destruction of the roof parapet, likely removed by metal scavengers to access the flashing and gutters. Mothballing is still feasible if the waterproofing envelope of the building is restored and wall vegetation removed. The Phase II ESA found asbestos in pipe and pipe fitting insulation, radiator and tank insulation, in the fire doors, floor tiles, and in roofing material. Asbestos abatement estimate: $768,890 (demolition) – $959,840 (renovation).
Glenn Dale Hospital Children’s Building, circa 2015
*
Gibson Hall, circa 2012
7b) Residence C Dormitory, “Gibson Hall”(1936, 2,849 sq. ft., map). 2016 Status: Still standing. This addition is the western of two wings which extend north from the Children’s Hospital Building. It is connected to the Children’s Hospital by an open-arched breezeway. A sun deck spans its entire roof and features a long pergola. The deck is accessed via the 3rd floor of the Children’s Hospital. A sleeping porch with broad, screened windows extends from its west elevation.
Some interior walls have collapsed, and its flat roof has not fared well, although the skeletal rooftop pergola remains. Asbestos was found in roofing materials and pipe insulation, asbestos danger is greater near the collapsed walls. Asbestos abatement estimate: $26,240 (demolition) – $35,300 (renovation).
Gibson Hall’s rooftop terrace has deteriorated rapidly: 2011 & 2016
Gibson Hall roof 2011Gibson Hall roof 2016
*
What’s left of Peabody Hall’s rooftop terrace.
7c) Residence D Dormitory, “Peabody Hall” (1936, 2,906 sq. ft., map). 2016 Status: Still standing.This addition is the eastern of two wings which extend north from the Children’s Hospital Building. A sleeping porch with broad, screened windows extends from its eastern elevation.
Like Gibson Hall, Peabody Hall is connected to the Children’s Hospital via an open-arched breezeway. It also has a sun deck along its roof, although its parapets and pergola have not survived. Asbestos was found in its roofing materials and in walls as pipe insulation. Asbestos abatement estimate: $26,480 (demolition) – $36,150 (renovation).
Western elevation of Peabody Hall.
*
Capper Hall, circa 2016 (courtesy Mike Perry)
8a) “Capper Hall”(1933, 22,888 sq. ft., map). 2016 Status: Still standing. Capper Hall was one of the earliest structures built at Glenn Dale. It was a dormitory for the nurses who tended to the children in the hospital.
It was built in 1933 and is loosely modeled after the Brice House in Annapolis, Maryland. A three-story central block is flanked by two smaller two-story gabled wings with perpendicular ends to create an H-shaped plan. In 1935 a
Capper Hall, circa 1989
brick arcade was added, extending from the southeast corner to connect the building to McCarren Hall, another nurse dormitory built in 1935.
The roof is in poor condition and the dormers are missing their windows, which has allowed water to penetrate the building. Vegetative growth rises inside the dormers on the side facing away from Glenn Dale Road.
To properly mothball Capper Hall the roof would need to be replaced and its floors would need to be secured from collapse. The Phase II environmental survey found Capper Hall contained asbestos-containing pipe insulation, pipe fitting insulation, tank insulation, and transite siding. Asbestos abatement estimate: $48,600 (demolition) – $64,700 (renovation).
Capper Hall, circa 1989
*
McCarren Hall, circa 2016 (courtesy Mike Perry)
8b) “McCarren Hall” (1935, 18,862 sq. ft., map). 2016 Status: Still standing. This was the second of two nurse dormitories built at Glenn Dale Hospital. Similar to its neighbor Capper Hall, McCarren Hall has a central three-story wing flanked by two smaller two-story wings.
A large two-story porch that once extended from its southern elevation has collapsed. The roof has failed in several areas, allowing water inside. To mothball, McCarren Hall would need its roof repaired and vegetation removed from the façade. Asbestos was found in floor tiles, mastic, transite siding, duct and pipe insulation, and in tank insulation. Asbestos abatement estimate: $134,900 (demolition) – $156,500 (renovation).
McCarren Hall’s porch before & after collapse
McCarran Hall with porch, circa 1989McCarran Hall without porch, circa 2012
*
West Duplex
9) Building F, “West Duplex”(1936, 5,673 sq. ft., map). 2016 Status: Still standing. One of two multi-family residences for physicians along the curved lane leading to the Children’s Hospital. Building F is the closest to Glenn Dale Road. It has two floors, a basement, and a detached two-bay garage. Wood-frame construction with brick veneer. The roof has failed in areas and the structure is in overall poor condition. Floor decking has rotted and water damage is evident.
To properly mothball the roof would need to be repaired and considerable re-framing will be required. Asbestos was found in pipe and tank insulation, floor tiles and mastic, and transite siding. Asbestos abatement estimate: $19,050 (demolition) – $22,475 (renovation).
West Duplex, circa 2016 (courtesy Mike Perry)
*
East Duplex
10) Building G, “East Duplex”(1936, 5,673 sq. ft., map). 2016 Status: Still standing. Very nearly a clone of Building F, Building G was also configured as a two-story + basement dwelling with a detached two-bay garage. The East Duplex has more vegetative overgrowth than the West Duplex. Some interior ceilings and walls have collapsed, exposing dangerous ACM in the pipe insulation and siding. Asbestos abatement estimate: $18,450 (demolition) – $21,625 (renovation).
East Duplex, circa 2016 (courtesy Mike Perry)
*
Aerial view of Finucane Hall (courtesy Bing maps)
11) Employee Dormitory Building, “Finucane Hall” (1938, 24,092 sq. ft., map). 2016 Status: Still standing. This employee housing structure is the westernmost building at Glenn Dale, sitting just southwest of the Adult Hospital. It was named for Glenn Dale Hospital’s first and longest-serving superintendent, Dr. Daniel Leo Finucane. The building’s relative seclusion on the campus has helped the three story (plus basement) building survive most of the site’s vandalism activity. There is cracking of the masonry along the roof parapets. The entire perimeter of the roof’s stone cap has been removed. The basement has standing water, and the steel railings and stairs are corroded.
Mothballing is feasible if the standing water is drained, the vegetation growing on its walls is removed, and a restoration of the waterproof envelope is performed. Some interior walls have been demolished, which has exacerbated the asbestos threat from pipe and tank insulation, floor tiles, and roofing materials. Asbestos abatement estimate: $185,200 (demolition) – $237,700 (renovation).
Finucane Hall circa 2016, western elevation. (courtesy Mike Perry)
*
The Adult Hospital’s open-air balcony (courtesy Mike Perry)
12) Adult Hospital Building(1936, 178,500 sq. ft., map). 2016 Status: Still standing. The largest building at Glenn Dale is the five-story, 400-bed Adult Hospital, which opened on September 17th, 1937. A semi-circular drive connects the U-shaped Adult Hospital with Glenn Dale Road. Like the Children’s Hospital, the Adult Hospital has rooftop terraces, and adds numerous balconies and sun rooms. The second and third floors feature sleeping porches, distinguishable by their large, wide screen windows.
As on the Children’s Hospital, the parapet of the Adult Hospital has been completely removed, likely the work of metal scavengers retrieving flashing. Otherwise the roof is in surprisingly good condition, however there is significant damage to the brickwork and masonry, and some interior walls have collapsed. Corrosion was found on interior beams and steel stairs, but overall the damage does not appear structural. To mothball the Adult Hospital would require restoring the waterproofing envelope and some masonry repair.
The Phase II ECA found significant asbestos in this building, citing the pipe and tank insulation, ceiling tiles, roofing materials, floor tiles, duct insulation materials, vibration dampers, transite hoods, conduit lining, and acoustical surfacing. Asbestos exposure is heightened in areas with demolished ceilings and walls. Asbestos abatement estimate: $1,744,790 (demolition) – $2,077,990 (renovation).
Aerial photo of the Adult Hospital building in 2012.
*
Paint and Repair Shop(1953, 1,157 sq. ft., map). 2016 Status: Still standing. Along with the Incinerator, the Paint and Repair Shop is considered a non-contributing structure toward the National Register’s designation. This white rectangular building is hidden behind the water tower and garage. Mothballing would be easier than the other structures, requiring only a restoration of the waterproof envelope; however it is not a contributing structure. Asbestos was identified on the pipe fitting insulation, transite ceiling panels, roofing materials, and window glazing. Asbestos abatement estimate: $3,750 (demolition) – $7,450 (renovation).
*
Incinerator
Incinerator(1960, 346 sq. ft., map). 2016 Status: Still standing. The incinerator was the last building constructed at Glenn Dale and one of two standing structures on the property that are not considered contributing to the “architectural significance and historical meaning” of the site as pertains to its National Register nomination. The incinerator contains asbestos in its roofing and transite siding. Asbestos abatement estimate: $2,000.
*
Collapsed, Demolished, & Incomplete Structures
Building D, “Doctor’s House 1”(1936, 4,610 sq. ft., map). 2016 Status: Demolished. This two story + basement home was one of four residences for physicians (two duplexes + two single-family dwellings) which lined the curving lane that led to the Children’s Hospital. Building D was later used as the superintendent’s residence. It was closest to McCarren Hall, and was lost in a fire in 1988.
A doctor’s residence at Glenn Dale Hospital, circa 1986. Today both are gone: One burned in 1988, the other in 2005.
Building E, “Doctor’s House 2”(1936, 4,610 sq. ft., map). 2016 Status: Demolished. This former single-family residence was another two-story plus basement home which also sat along the curved street which leads to the Children’s Hospital. Like Building D, Building E was also lost in a fire – this time in 2005.
Hot House(1948, 823 sq. ft., map). 2016 Status: Collapsed. A debris pile was all that remained of the hot house, which once sat directly behind the pump house. Even the debris contained an asbestos threat, as the Phase II ECA found contaminated window glazing in the collapsed pile. Asbestos abatement estimate: $2,000.
Sludge Bed Enclosure(1936, 886 sq. ft.). 2016 Status: Collapsed.
Sedimentation and Control Building (1936, 1,905 sq. ft.). 2016 Status: Collapsed.